kaiser permanente appeal form
Street City Zip Code Daytime Telephone Number. Appeal Decision Timelines.
Fillable Online Info Kaiserpermanente Medicare Grievance Form Info Kaiserpermanente Fax Email Print Pdffiller
If you need an expedited appeal due to a life-threatening situation call us.
. Health Care andor Financial Dependent Power of Attorney form stipulating you are currently authorized to appeal on behalf of the member. Provider reconsideration process The claims payment review and reconsideration steps include. How to answer member questions or concerns about the way a claim was processed by Kaiser Permanente in the Northwest.
Kaiser Permanente Signature. Request status approved partial approval or denied will be communicated directly to the requesting provider the referred-to. Please return form to.
Sign in to the secure Kaiser Permanente member website and submit the Online Member Appeal Request. Mid-Atlantic Claims Administration Kaiser Permanente. How soon should surgery take place.
Kaiser Permanente Member Appeals PO. File a complaint grievance or appeal about Kaiser Permanente Part D drug or the care you received without fear of retribution or discrimination expect problems to be. Return completed form to.
Seattle WA 98124-1593 ATTN. Each covered family member may designate a different PCP. Submit your request for a standard appeal in writing by fax mail or online through the Kaiser Permanente member website see below for contact information.
Information on how to submit changes or updates to your provider information so Kaiser Permanente can maintain an accurate provider directory. Find forms for health services billing and claims referrals and clinical review behavioral health services provider information and more. Appeals procedures for members in the Mid-Atlantic States region.
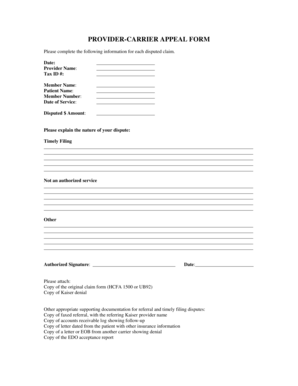
How to Appeal Mail PO. Appeal is submitted without Appeal Filing Form the information listed below must be present. Kaiser Foundation Health Plan Inc in Northern and Southern California and Hawaii Kaiser Foundation Health Plan of Colorado Kaiser Foundation Health Plan of Georgia Inc Nine Piedmont Center 3495 Piedmont Road NE Atlanta GA 30305 404-364-7000.
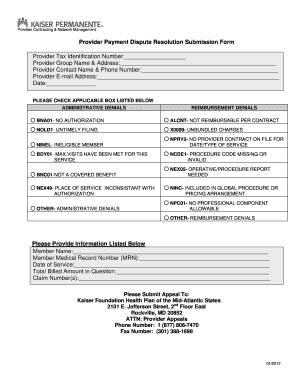
Box 372970 Denver CO 80237 PROVIDER- CARRIER DISPUTEAPPEAL FORM Please complete the following information for each disputed claim Date. GrievanceAppeal FORM - Medicare Southern California MemberPatient Name. HMO- Center-Based PCP.
Please note that all claim payment appeal requests must be filed within 365 days of the date the claim was originally processed or denied in order to be considered for payment by Kaiser Permanente. An inventory of all forms for health services billing and claims referrrals clinical review mental health provider information and more. Appeals procedures for members in the Hawaii region.
Kaiser Permanente Health Plan Coverage Options. Print this form and fill in the information if your doctor recommends that you have a surgical procedure. Why do I need surgery.
Customize the template with unique fillable fields. Kaiser Foundation Health Plan of the Northwest Member Relations Department 500 NE Multnomah St Ste. Enrollment forms request the designation of a PCP from the Health Plans provider directory for each enrollee.
Complete the Member Appeal Request form PDF and return it to the Member Appeals department using one of the following delivery options. Name of Person Filing If. Original Claim Amount Billed.
Kaiser Permanente health plans around the country. Medicare Advantage Appeals Process Level WrittenVerbal Resolution Maximum timeframe from contact date not including extensions. Original Claim Amount Paid.
Claims disputes Member appeals. Appeal Submission Address for Coverage Plans Listed Below. Box 34593 Seattle WA 98124-1593.
Appropriate Appeal Submission Addresses. 100 Portland OR 97232 Fax 1-855-347-7239. What might happen if I delay or avoid the surgery.
Member Relations Grievance and Appeal Form Author. Kaiser Permanente Provider Appeals Provider Contracting and Relations 500 NE Multnomah Blvd Ste 100 Portland OR 97232 503-813-3376 503-813-2017 Fax. GrievanceAppeal FORM - MedicareSouthern California.
Kaiser Permanente health plans around the country. Kaiser Permanente Medical Record Number. General questions What is the name of the surgical procedure.
If you are the treating provider submitting this request on behalf of a member you must submit an. How to appeal claims as a provider for members in the Northwest region. You contact our health plan and make your appeal.
Fill in the empty fields. Kaiser Foundation Health Plan Inc in Northern and Southern California and Hawaii Kaiser Foundation Health Plan of Colorado Kaiser Foundation Health Plan of Georgia Inc Nine Piedmont Center 3495 Piedmont Road NE Atlanta GA 30305 404-364-7000 Kaiser. You may now submit online disputes or appeals online via the Online Affiliate portalSign-On or register to access KP Online Affiliate and start using this feature today.
Include the particular date and place your electronic signature. Involved parties names addresses and phone numbers etc. Kaiser Permanente Claim ID Number.
KP HAWAII PROVIDER APPEALS CLAIMS ADMIN DEPT PO BOX 378021 DENVER CO 80237-9998. Open it up with cloud-based editor and start adjusting. Then you must send Kaiser Permanente Member Appeals.
Get the Kaiser Permanente Appeal Form you need. If you disagree with the handling of a claim you should first call Member Services at 301-468-6000 to inquire about the claim. Call Member Appeals Toll-Free 1-866-458-5479.
Reason for denial member name medical record number service dates and. Signature Select Added -Choice Flexible Choice Option 1 Medicare Advantage and Medicare Plus. Downloading forms at your convenience saves you time.
Patient Date of Birth. Kaiser Permanente of Colorado Provider Appeals PO. HMO- Center or Network-Based PCP.
To ensure a quick response be certain to choose the correct form complete it fully and carefully and use the correct FAX number.
Group Election Request Form Northern California Or Southern California Region

Kaiser Permanente Doctor Note Doctors Note Template Doctors Note Notes Template
Kaiser Permanente Combined Disclosure Form At Your Service
Kaiser Permanente Grievance Form Southern California 2020 2022 Fill And Sign Printable Template Online Us Legal Forms
2
2
Get And Sign Kaiser Permanente Work Status Report Pdf Form
Application Kaiser Permanente California

Fillable Online Info Kaiserpermanente 2020 Kaiser Permanente Silver 70 Hmo 2500 45 Fax Email Print Pdffiller
Application Kaiser Permanente California
Claims 8 0 Kaiser Permanente

Kaiser Permanente Rejecting Some Religious Exemptions To Employee Covid Vaccine Mandate Fox 5 San Diego
Kaiser Provider Appeal Form California Fill Online Printable Fillable Blank Pdffiller
Fillable Online Info Kaiserpermanente Provider Carrier Appeal Form Kaiser Permanente Info Kaiserpermanente Fax Email Print Pdffiller

Kaiser Permanente Doctor Note Check More At Https Nationalgriefawarenessday Com 30691 Kaiser Permanente Doc Doctors Note Template Doctors Note Notes Template
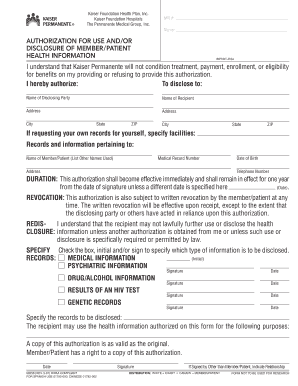
Fillable Online Mydoctor Kaiserpermanente Kaiser Permanente Authorization For Use Or Disclosure Form Fax Email Print Pdffiller
![]()
Kaiser Permanente Of Washington Options Washington State Health Care Authority
Kaiser Permanente Ns 1062 2003 2022 Fill And Sign Printable Template Online Us Legal Forms
2